Philosophy as Therapy
A Review of Konrad Banicki’s Model in Philosophical Papers, Vol.43 (2014), No.1, 7-31
Bruno Contestabile and Michael Hampe November 2015
Table of Contents
1. Therapeutic Goals
2. Therapeutic Methods
3. Efficacy
4. Semantics
5. Chances and Risks
6. Historical and Cultural Context
7. Relation to Psychotherapy
8. Relation to Religion
In his article Banicki proposes a universal model for all forms of philosophical therapy. He is guided by works of Martha Nussbaum, who in turn makes recourse to Aristotle. As compared to Nussbaum’s approach, Banicki’s model is more medical and less based on ethical argument. He mentions Foucault’s vision to apply the same theoretical analysis for the ailments of the body and the soul and to use the same kind of approach in treating and curing them. In his interpretation of philosophical therapy, there are, however, some controversial issues, to which we would like to call attention:
Is restoring health by a philosophical method of treatment – health understood as a person’s ability to reach his/her vital goals – a convincing explication of philosophical therapy in general? In order to answer this question it may be useful to look at Plato. It is not only Platonism (and especially Neo-platonism since Plotinus) that questions the idea that therapy is necessarily connected with „vital goals“. Buddhist and Gnostic philosophies are questioning „the vital“ in general. The immense effort in the history of philosophy to liberate the mind from the body casts doubt on the project to explain philosophical therapy solely in analogy to medical therapy.
According to Banicki a therapeutic philosophy has to identify the diseases it attempts at curing. There are, however, reasons for associating the term therapy with suffering/risk rather than disease. If a therapy aims at reducing the fear of death, as for example many classical philosophical therapies do, then there is no disease to be cured. A model based on chances and risks also has the advantage that the Buddhist and Stoic reinterpretation of desires/emotions as “diseases” can be dropped in contemporary philosophical therapy.
Banicki mentions the comparison of therapies as one of the primary goals of modelling. Methods should be verified by a statistical correlation between method and therapeutic success and/or by a theory which justifies the method. Some forms of therapies, however, avoid theory-specific terms and concepts in favor of an unprejudiced interpretation of the patient’s statements. Others share the (Nietzschean) aspiration to explore and change measures of value. If the therapeutic process is seen as a unique phenomenon, then there can be no theory and no statistics with co-occurrences.
According to Banicki philosophical therapy has to describe techniques which qualify as genuinely philosophical. Techniques like maieutics and hermeneutics, however, are antique philosophical “inventions”, which were later adopted by psychotherapy. If meditation is accepted as a therapeutic tool – as it was in ancient times – then there is not only a methodical but also an emotional relation to religion. If finally the Socratic search for a good life is seen as one of the characteristics of philosophical therapy, then delimitation even turns into a criterion for non-philosophical therapies. The search for a good life requires an interdisciplinary approach.
For the concretization of the formal structure we suggest a typology of therapies, which is based on chances and risks. Such a typology has the advantage, that it can model conflicting (and even opposing) forms of therapies. The variety of therapeutic goals and methods is a consequence of the historical development towards conceptual freedom.
A PDF-version of this paper is available from
Is restoring health by a philosophical method of treatment – health understood as a person’s ability to reach his/her vital goals [Banicki, 15-16] – a convincing explication of philosophical therapy in general? In order to answer this question it may be useful to look at Plato. Already in the Apology Socrates refers to the importance of caring for the state of the soul (passage 29e, Banicki refers to the Apology on page 20). At the end of the Phaedo, when Socrates has swallowed the poison, his last words are: „Crito, we owe a cock to Aesculapius. Pay it and do not neglect it“ [118a, Plato I, p. 403]. One possible interpretation of this passage is that Socrates wants a sacrifice to the God of medicine because he considers his death as a salvation from suffering [Taylor, 12]. In his last dialogue he tries to prove the immortality of the soul and the problematic status of its existence in a desiring and suffering body. Thus death can be seen in this Socratic perspective as a therapy of the soul: it is not caught anymore in a body, but free to see truth itself. Such an interpretation would have nothing to do with „vital goals“, „survival and reproduction“ or “curing a disease” [Banicki, 14-16]. Nevertheless it has to do with philosophical therapy since therapy is for Socrates primarily concern about the soul or the Gods [cf. Ritter 1998, Vol 10, p. 1163a]
It is not only Platonism (and especially Neo-platonism since Plotinus) that questions the idea, that therapy is necessarily connected with „vital goals“. Buddhist and Gnostic philosophies are questioning „the vital“ in general. The fact that Nietzsche conceived the affirmation of life as something mankind will achieve in the future (cf. Zarathustra´s metaphor of the Christian camel, the nihilistic lion, and the child of the postnihilistic age) indicates that he considered a positive valuation of „the vital“ in his times as a rarity. He reacts actually against Christian and Buddhist (Schopenhauerian) negative evaluations of the physical life as characterized by unavoidable suffering. Salvation from an existence that is bound to vital goals was an aim of Christian and Buddhist therapy, which – in the Age of Reason – Nietzsche considered leading to Nihilism. His therapeutic efforts were therefore directed towards an approval of the vital goals. But this makes only sense, if such an approval was not self-evident in his time.
Historically philosophy went on distance to vital goals, when it pursued a soteriological mission, closely affiliated with religion. Knowing the “supreme reality” means knowing the path to the liberation from suffering – that is the claim of the rationalist Hindu philosophy (Samkhya), which could be at the root of Buddhism [Baus 2006, 43-44]. As a result there are (at least in a very rough classification) two contradictory goals of philosophical therapy:
1. A strategy which upgrades vital goals/human flourishing [Banicki, 17] and attempts to cope with suffering.
2. A strategy which – conversely – devaluates earthly life and aims at the liberation from suffering.
Samkhya, Buddhist, Platonic and Gnostic philosophies, as well as parts of modern antinatalism are examples for the second strategy. They all devaluate material desires and search for a spiritual resort. Hindu monks believe that nothing detracts the human soul more from the path of liberation than the birth of a child, a view that accords well with the scientific (genetic) conception of reincarnation. Childlessness is also the consequence of “Platonic love” – the endeavor to transcend physical love. From a contemporary perspective the spiritual world does not exist in the hereafter, but in the brains of all philosophers who strive to liberate the mind from the body. Individuals come and go, but the idea of a world free from suffering remains. The (imagined) liberation from suffering is a possible source of well-being, just as well as the kind of happiness that goes with life’s biological destination. In the following we will use the term retreat-oriented for this type of therapy. It can – but does not have to – go with a retreat from public life.
How can retreat-oriented therapies be included in the definition of philosophical therapy? Obviously the term survival and reproduction which characterizes the paradigm of somatic medicine, as well as the term treatment of a disease in the sense of the World Health Organization [Banicki, 14-16] are not adequate. We have to look for a common characteristic of all practices:
Life-affirming and retreat-oriented therapies meet in the common goal to cure (or reduce) suffering.
The reduction of suffering is less ambitious than the WHO’s complete physical, mental and social well-being [Banicki, 16], but probably more realistic. Do we not expect too much from philosophical therapy, if we aim at complete well-being?
Admittedly the history of philosophy is full of happiness promoting ethics like the one of Aristotle and Spinoza. (In this context we use the term happiness as a synonym for well-being). We have to ask, however, if the ideal of complete well-being is therapeutically helpful at all. The deliberate attempt to become happy often generates a counter-productive result. In Western societies happiness has become a right to happiness and a kind of coercion [Hettlage 2002, 154]. People are unhappy for not being (perfectly) happy.
Spinoza commented that his concept – although logically impeccable – is difficult to realize [Spinoza 2002, p. 382, Vp42s] and interestingly, the origin of the term eudaimonia relativizes the controllability of well-being too. In some ancient Greek traditions successful and happy persons were thought to be protected and promoted by a daimon (guardian spirit) and we may assume that Aristotle was well aware of these conceptions when he used the term. Sigmund Freud, who puzzled over contemporary interpretations of the Greek demons, clarified that well-being not only depends on factors like talent, social environment and contingent events in one’s life story, but also on the irrational forces of the unconscious. Well-being can be influenced, but not controlled.
We agree with Banicki’s view that somatic and behavioral techniques should be accepted in philosophical therapy [Banicki, 12-13]. According to Spinoza´s double aspect theory every change in the mind will also be a change in the body (and vice-versa). Following the reasoning of his Ethica [Spinoza 2002, p. 251 & 259, IIp13 & 21] – which can be understood as a philosophical therapeutic enterprise [Hampe 2010] – will accordingly not only change the reader´s mind but also his/her body. It is well known from Plotinus and from the Stoics that they considered physical exercises like fasting and sleeping in hard beds as much as a part of their philosophical therapies as discussing and contemplating [cf. Hadot. 1995, Ch. IX]. The distinction between reasons and causes is a clear and widespread one in contemporary philosophy. But philosophical therapy is reduced to a discursive cognitive exercise, if one accepts only those practices that deal with reasons.
Another question is, if psychotherapeutic techniques should be applied in philosophical therapy. According to Banicki philosophical therapy has to describe techniques which qualify as genuinely philosophical and explain their efficacy in curing the disease [Banicki, 16]. The definition of techniques which are genuinely philosophical, however, is a controversial issue because ancient techniques like maieutics, hermeneutics and the change of perception are used in psychotherapy as well as in philosophical therapy. One could – conversely – ask psychotherapy to demonstrate that their methods are genuinely psychotherapeutic; a difficult enterprise if one considers that in ancient times the boundaries between philosophy and psychotherapy were inexistent since a medical discipline “psychotherapy” did not exist. From a historical perspective there is no compelling reason, why philosophical therapy could not work in conjunction with psychotherapy.
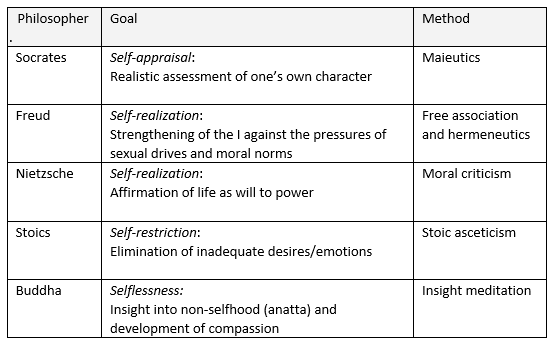
The following table shows a rough classification of therapeutic goals and corresponding methods:
- Buddha explored topics in phenomenology, ethics and epistemology and can therefore be seen as an ancient philosopher. The four-fold structure of a therapy [Banicki, 15] is exemplarily modeled in the four Buddhist truths: diagnosis, etiology, prognosis, and prescription [Gethin 1998, 63-64].
- The philosophical significance of Freud’s psychoanalysis was investigated by Stanley Cavell [Cavell 2004, 289-295, Hampe 2006]. Philosophical psychoanalysis is practiced on the basis of free association and hermeneutics, without using an expert language and without being fixed on Freudian concepts like the Oedipus complex.
Since the 1980s there is a movement within practical philosophy under the name philosophical counseling, which developed new forms of individualistic therapies [Achenbach] [Marinoff][Raabe] [Schuster][Van Deurzen].Therapeutic concepts are adapted to the patient rather than interpreting the patient’s statements in terms of a theory.
At about the same time started the investigation of meditative techniques in psychology and psychiatry [Delmonte][Smith][Goleman]. Ancient Indian techniques for modifying emotions are quite different from cognitive approaches [Banicki, 24-25]. According to Buddhist schools intellectually understanding that everything comes into being and passes away is much too superficial in order to heal a person from the fear for death. One has to experience the transience of the self in a calm, anxiety-free mood. This can be achieved by meditating for a long time: sensations, thoughts, pains come and go. The meditator contemplates them and does not react to them. But he sees clearly: everything he experiences arises and passes away. The understanding that is reached by this bodily practice is „deeper“ than that which can be reached by reading a text or having a discussion. An evidence is produced, like the one that stems from other perceptions: Hearing reasons for the fact that it is raining does not lead to the same kind of „unshakeable“ conviction as the experience of seeing drops falling from the sky and feeling how they hit the skin.
An example for the cognitive approach can be found in Epicurus’ letters to Meneoceus:
“Become accustomed to the belief that death is nothing to us. For all good and evil consists in sensation, but death is depriving of sensation… So death, the most terrifying of ills, is nothing to us, since so long as we exist death is not with us; but when death comes, then we do not exist. It does not concern either the living or the dead, since for the former it is not, and the latter are no more.” [Epicurus, 30]
A formal analysis of therapeutic methods also has to consider the different forms of communication. There is the real personal dialogue, the written dialogue (Plato), the moral lecture (Aristotle´s Ethics), the letter (Seneca), the consoling book (Boethius as dialogue, Kierkegaard), the meditation (Descartes), the essay (Montaigne), the proving system (Spinoza). They all include arguments. But they deal with them differently and they are based on different ideas about their effectiveness. The cognitive therapy Banicki is referring to via Fischer [Banicki, 7-8, 26-27] is only one possibility.
Banicki mentions the comparison of therapies as one of the primary goals of modelling [Banicki, 13]. His application examples are historical examples and his motivation for comparing therapies seems to be a purely academic one [Banicki, 22-25]. There is, however, a strong economic interest of health insurances to test and compare the efficacy of therapies. The basic questions
- Is a certain form of therapy effective and – if yes – how can efficacy be measured?
- Is therapy A more effective than B?
have a scientific touch – they sound like scientific questions – but the terms used here cannot be defined operational and binding for all (as in physics) [Kriz 2000, 8]. The demand for a statistical correlation between method and therapeutic success is accordingly disputed [Banicki, 17].
The alternative demand for a theory (supporting the method) is not generally enforceable as well. Some forms of therapies avoid theory-specific terms and concepts in favor of an unprejudiced interpretation of the patient’s statements [Van Hooft 2003, 20]. Others share the (Nietzschean) aspiration to explore and change measures of value. For some schools of contemporary philosophy that are committed to the ideals of enlightenment freedom of thought is the main goal of philosophical activity. If the therapeutic process is seen as a unique phenomenon, then there can be no theory and no statistics with co-occurrences.
There is, of course, a concern that non-measurable and non-comparable methods serve the incompetent therapists. On the other hand incompetent therapists will also measure and compare therapies in an incompetent manner. The problem can probably only be solved by a competent supervision.
A different question is, if the importance of psychological theories, techniques and jargons is not generally overestimated – in particular if there are no specific symptoms. Possibly non-quantifiable factors like experience, empathy and “interpersonal chemistry” decide about the success of a therapy [Kriz 2000, 20]. If that is true, then the task rather consists in collecting information about therapists than about methods.
According to Banicki the structure constituted by the three concepts health ideal, disease and process of treatment seems to be generally accepted in thinking about medicine or therapy of any kind [Banicki, 14]. Consequently he demands that a therapeutic vision of philosophy has to identify the diseases it attempts at curing [Banicki, 15]. There are, however, reasons for associating the term therapy with suffering/risk rather than disease:
- If a philosophical practice aims at reducing the fear of death – as in our example with Socrates – then there is no disease to be cured. Patients often have to decide between a longer, painful life and a shorter, higher-quality life, when they are confronted with the physicians’ estimations of “quality-adjusted life years”. A practice, which helps accepting the inevitable dissolution of the self, is fundamentally different from a practice, which aims at survival. But (given a rational world view) both have finally to be brought down to the common denominator suffering/risk [Aizawa 2013].
- Similarly in couple therapy, it may be hard to identify a mental disease to be cured. After having reached a deeper understanding of the problem, the outcome of a therapy is often – particularly in the case of an impending divorce – a choice between different forms of suffering/risk.
- Philosophical therapists may be confronted with the existential despair, which is caused by the loss of religious (and secular) scenarios of salvation. The search for meaning in life is not necessarily the symptom of a mental disease.
- Finally, the term “palliative therapy” demonstrates that even in medicine the term “therapy” is sometimes associated with the reduction of suffering and not with the “cure of a disease”.
Obviously, there are two competing definitions of the term “therapy”:
1. a narrower definition, where therapy is understood as the cure of a disease
2. a wider definition, where therapy is understood as a cure (or reduction) of suffering.
Under the assumption that a disease always goes with some kind of suffering (at least if we include the patient’s social environment) the cure of a disease is also a cure of suffering. The two definitions even match, if suffering itself is seen as a disease. An example for the latter case is Buddhism [Gethin 1998, 63-64].
In Stoicism specific desires/emotions are compared with infirmities of the body:
“And as there are said to be certain infirmities in the body, as for instance gout and arthritic, so too there is in the soul love for fame, love for pleasure, and the like (…). And as in the body there are tendencies to certain maladies such as cold and diarrhea, so it is with the soul, there are tendencies like enviousness, pitifulness, quarrelsomeness, and the like.” [Laertius, 221]
Banicki’s uses a radical interpretation of Stoicism:
“The sole identification of the disease with pathé, however, is far from sufficient for the purposes of establishing Stoicism as a literal therapy. What is still needed is to show that emotions, and in the case of the Stoics these are all emotions, can be intelligibly considered as diseases.”[Banicki, 23]
The association of the term Stoic with unemotional, and apathetic with the “absence of all emotions”, however, is a change of semantics relative to the original meaning. According to Donald Robertson the focus of Stoicism was more on stopping to make false judgments, than on repressing emotions [Robertson 2013]. Emotions were perceived as judgments, which can either be right or wrong. Wrong emotions express suffering directly (like grief and fear) or they lead to suffering indirectly (like craving and pleasure) [Laertius, 217-220]. The latter judgment expresses – similar to Freud’s reality principle – the result of a long-term rational view.
Not all emotions were considered to be wrong. Diogenes Laertius – who refers to the founders of Stoicism – mentions three emotions which are “right”, namely joy, caution and wishing:
Joy, the counterpart of pleasure is rational elation. Caution, the counterpart of fear, rational avoidance (…). And they make wishing the counterpart of desire (craving) inasmuch it is rational appetency [Laertius, 221].
A statement which deserves special attention is the following:
…in another sense the term apathy is applied to the bad man, when it means that he is callous and relentless [Laertius, 221].
To be emotionless can be right or wrong, depending on the context – ethical knowledge makes the difference. Ethical knowledge is knowledge about human nature. Nature is driven by rational laws and living in accordance with these laws – by making reasonable judgments – is the Stoic path to the avoidance of suffering.
The origin of the Greek word apatheia has a strong connotation with the “avoidance of suffering”: a- means "without" and pathos means literally “what befalls one”, related to paskhein "to suffer," and penthos "grief, sorrow;" from the Proto-Indo-European root *kwent(h)- "to suffer, endure" [Harper 2015], [Harbsmeier & Möckel 2009].
Why not interpret Stoicism as a therapy, which liberates people from the suffering, which is caused by unreasonable judgments? Such an interpretation would also conform to the thesis that Stoicism was inspired by an older philosophy, which pursued the liberation from suffering by means of knowledge [Baus 2006, 8].
Whereas the notion of “wrong desires/emotions” changes considerably in the course of history, the goal to reduce suffering by means of knowledge is vastly undisputed and survived all times. With regard to contemporary philosophical therapy it is therefore recommendable, to apply the wider definition of therapy. The reinterpretation of desires/emotions as “diseases” in Buddhism and Stoicism is first and foremost of historical interest.
If we adopt the wider definition of “philosophy as therapy”, then the variety of therapeutic concepts can be seen under the aspect of the chances and risks which are caused by attachments. Buddhists, Cynics and Epicurus, for example, developed a strategy to reduce risk by reducing social commitments. If Stoics are socially engaged [Laertius, 225-226] then by duty or altruism, but not by passion. This reduction of emotional risk has to be paid by the loss of “natural” happiness. Aristotle used the argument that insensitiveness is far from human nature [Höffe 2006, 101]. But Buddhists and Hellenists are not insensitive, they are differently sensitive. The question is whether meditative, contemplative and altruistic kinds of happiness can compensate the loss of passionate kinds of happiness [Nussbaum 1994]. Some meditators report that they undergo phases of anxiety and depression during their practice. The success of meditation depends on the ability to sit out (in a literal sense) such critical phases. The sublimation of passion is hard work and – like any other philosophical therapy – not suitable for everybody. If the compensation of passionate happiness fails, then Buddhist and Hellenistic therapies – while avoiding external risks – start to create internal risks. If the compensation succeeds, then the passionate life looks like a questionable risk.
Philosophical therapy is concerned with the suffering/risk caused by desires (Buddha, Stoics) as well as the suffering/risk caused by the repression of desires (Nietzsche, Freud). The boundaries between “ordinary suffering” and suffering from mental disorders (diseases) are fluent and depend on the cultural and historical context [Devereux 1974]. Following two examples:
1. Cynics, who strive for an ascetic and natural life, consider the average citizen’s struggle for power and wealth to be foolish. Conversely Nietzsche describes the renunciation to power as a perversion of human nature and as an invitation for social suppressors. Both philosophies tend to associate dissident behavior with a mental disease.
2. The early Buddhists understood suffering in general as a disease, the Eightfold Path as a cure and Buddha as a healer. The average citizen’s struggle for procreation – seen from this perspective – corresponds to a collective delusion. Conversely, wandering ascetics like the early Buddhists are often considered to be fools. A sexual behavior according to Buddhist standards corresponds to a neurotic disorder according to Freud’s standards. Psychoanalysts – who claim the role of healers as well – consider the Buddhist medicine to be worse than the disease.
Declaring a certain behavior to be a disease is a strong normative claim. But from an ideology-free perspective none of the persons in question is mentally ill. They simply adhere to different world views and pursue a different sense in life. Each sense (chance) is tied to specific risks and therapies are only required, if the pressure of suffering becomes too high. In the latter case seemingly fateful kinds of suffering may prove to be avoidable by changing the way of living.
In our view contemporary philosophical therapy should not distinguish between different mental diseases – that is the task of psychotherapy – but between different kinds of suffering/risk, caused by different ways of living.
6. Historical and cultural context
Retreat-oriented therapies emerge in times of war or social suppression. Buddhism can be seen as a reaction to the suppression by Zoroastrian [Beckwith 2015, 178] and Brahmanic orthodoxy and the Gnosis as a reaction to the suppression of the early Christians. The proliferation of Buddhism across Asia is attributed to the conversion of the Indian emperor Ashoka, after he had witnessed the mass deaths of the Kalinga war [Bentley 1993, 44-46].
Philosophical therapy also gains importance in times of ideological uncertainty. The Hellenistic therapies for example emerged from the conflict between the representatives of the antique pagan world view and their critical-rationally arguing challengers. Philosophers who specialized on ethics like Socrates, Pyrrho, the Cynics, the Stoics and Epicurus adopted a therapeutic function, which the priestly caste was not able to exercise. Among these therapists the Cynics, Pyrrho and Epicurus belong to the philosophers, who went on distance to the risks of family life.
An example from the US American present is the conflict between the future-oriented movement of transhumanism [Bostrom 2005] and the retreat-oriented movement of antinatalism [Benatar 2006]. The former quest for eternal life despite of the risks, the latter – conversely – devaluate survival because of the risks. Transhumanism is supported by the claim that humanity without the perspective of future happiness would fall in a deep depression and that “we” are therefore forced to think positively [Scheffler 2015]. With regard to the biological fitness the retreat-oriented therapies should indeed have disappeared long time ago. The fact that they still exist prompts the conclusion that negative valuations steadily emerge anew, because obviously the corresponding reasons do not die out. Nietzsche suspected that retreat-oriented philosophies can be explained by the distorted perception of suffering people:
“Summarized: the world, as it should be, exists; the world we are living in is only a delusion, - this (our) world should not exist (…). What kind of people think like that? An unproductive, suffering kind; a suicidal kind” [Nietzsche 1885, 402].
The argument that the perception of the world is distorted by individual sensitivities, however, can be applied to Nietzsche’s view as well. From the Buddhist perspective the vital goal “to survive and procreate” (respectively Nietzsche’s “will to power”) causes the major distortion, because it makes us think that survival justifies the immense suffering in this world.
Life-affirming and retreat-oriented philosophies are in a permanent battle for interpretive predominance – with life-affirmation in the advantage for obvious reasons [Contestabile 2014, 304-310].
The goal to survive and the fight against suffering not only compete within cultures, but also within the psyche of individuals. The coexistence of contradicting aims in life can probably best be illustrated from the example of Hinduism [Zimmer 1973, 44-50]. The life-affirming goals Kama (lust and love), Artha (power) and Dharma (law-abidance) are confronted with the unworldly goal Moksha (salvation), i.e. with the aspiration to escape from the painful circle of reincarnation. The shift of the weight, which is given to these goals in the course of life, is described in the Ashramas (stages of life). The claim that well-being in the last stage of life can be improved by changing ethical priorities has been investigated empirically [Lelkes].
There is a historical development from normative therapies (Buddhism, Stoicism) to more individualistic therapies (Nietzsche, Freud). The focus – which was on the control of desires – shifted to the liberation of desires. Obviously in ancient times the main risk was to be misguided by passion, whereas therapies according to Nietzsche and Freud make clear, that the repression of passion is a risk as well. A contemporary philosophical therapy disposes of a rich inventory of divergent (and even opposing) methods which can be adapted to the patient’s individual environment and risk-profile. The history of therapeutic philosophy is a movement towards conceptual freedom. Philosophical counseling, which partly uses philosophical concepts like a toolbox, marks the tentative peak of this development.
We do not expect from psychotherapy that it reflects its historical and cultural context. But what else does it distinguish from philosophical therapy?
That largely depends on the definition of philosophy [Banicki, 26-27]. If philosophy is not only seen as an intellectual activity, but also as a way of living [Hadot 1995], then it is suited to develop therapeutic techniques as well as psychotherapy. But – from a historical perspective – the techniques of philosophical therapy were first of all developed for the worries of mentally sane people, whereas the techniques of psychotherapy were first of all developed for mentally ill people.
Although it is difficult to draw a line between sanity and mental illness, it can be said that the focus of philosophical therapy is not on mental disorders like eating disorders, anxiety disorders, schizophrenia and major depression. The Diagnostic and Statistic Manual of Mental Disorders (DSM), published by the American Psychiatric Association is therefore a possible demarcation line between psychotherapy and philosophical therapy. The main concern of philosophical therapy is to reduce the suffering of mentally sane people, by improving their knowledge about (repressed) risks and chances.
A different criterion for the delimitation of philosophical therapy from psychotherapy is the search for the “objectively” true and good [Banicki, 27] [Van Hooft 2003, 28]. This search requires an interdisciplinary approach – which was self-evident in the antique – whereas psychotherapy is a specialized field within the social sciences. The separation began with the development of individualistic therapies:
“As a specialized science, a branch of psychology – ‘depth-psychology’ or psychology of the unconscious – it is quite unsuited to form a “Weltanschauung” of its own; it must accept that of science in general” [Freud 1933, 128].
But the world view of science does not answer the questions about the meaning of life – at least not in a traditional sense. A contemporary philosophical therapy is therefore confronted with the kind of cultural pessimism that emerges from the loss of religious (and secular) scenarios of salvation [Van Hooft 2003, 22]. Philosophical therapy and psychotherapy both have a potential to create sense in life by disclosing repressed chances. But philosophy – with its millenniums-old tradition in reflecting existential questions – may be in the advantage.
Science also does not answer the question “What is a good life?” For that reason normative ethics belongs to the few areas of philosophy which have not been challenged by specialized sciences. Whereas psychotherapy delegates economic and political questions to separate disciplines, philosophy works on normative answers. Philosophy may e.g. ask if it were not more efficient to improve the living conditions than to occupy therapists with the result of an oppressive environment. If the notion of justice is extended beyond the civil law, then the conflict between subjective and “objective” interests moves in the focus of attention. This kind of questions however, is rather raised at the end of a therapy than at the beginning [Van Hooft 2003, 28].
The search for the “objectively” true and good is a relatively undisputed criterion for the sought-after delimitation. More challenging is a delimitation based on methods. Many of the actual methods in psychotherapy have their origin in the philosophy of the antique. Among them are maieutics, hermeneutics and the change of perception. Philosophy as a way of living also does not exclude meditation. This wide definition of philosophy is nowadays disputed, but it was not unusual for antique Indian and Greek philosophers [Hadot 1995]. Since about the 1980s there is an increasing interest in psychotherapy to explore meditative techniques.
The following table shows a rough classification of methodical relationships:
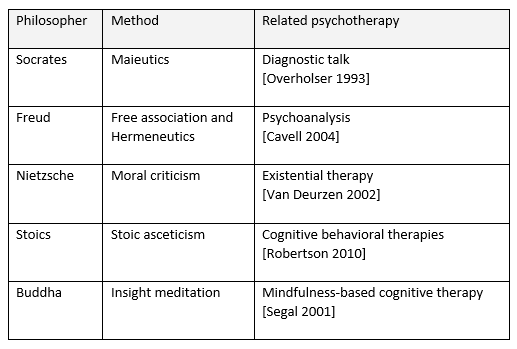
Although it seems possible to find criteria (like the DSM) for the delimitation of philosophical therapy and psychotherapy, there is also a strong argument for cooperation: the boundaries between “ordinary” suffering and suffering from mental disorders are fluent.
Concerning the relation between philosophy and religion Banicki maintains that they are close in aiming at the truth, but easily separable from a methodical point of view [Banicki, 27].
Does religion aim at the truth indeed?
The question could be answered positively insofar, as some Hindu philosophies are hard to separate from religion and their history seems to mirror a deeply felt struggle for truth [Zimmer 1973]. It is implausible, however, to associate revealed religions like Judaism, Christianity and Islam with the search for truth in the same sense as philosophy. The kind of truth that is found by revelation is not comparable to the truth that is found by a Socratic search. Conflicts like the one between the theory of evolution and creationism show exemplarily that the revealed religions’ truth claim is hard to reconcile with the philosophical conception of truth.
Are philosophy and religion easily separable with regard to their methods?
On the one hand philosophy denies faith and revelation as means to acquire knowledge. Philosophy-specific methods already emerged in ancient Hinduism and Buddhism, independent from metaphysics, meditation practices and rituals, anticipating many of the later developments in Western philosophy [Lorenz 1998].
On the other hand there are also far reaching commonalities. Historical research has shown that the religious-philosophical tradition of ancient India strongly influenced Greek philosophies like Platonism, Pyrrhonism, and Stoicism, to mention only a few [cf. Beckwith 2015, Kuzminski 2008, McEvilley 2002]. Practices of contemplation were as much transferred from the East to the West as propositional theories [cf. McEvilley 2002, Ch. 6]. Furthermore the methods of revealed religions are not restricted to faith and revelation. If once the dogmas are set, theology reasons logically as well as philosophy. Already the medieval scholasticism – which was structured in its thought deeply by the writings of Aristotle – used techniques like deduction, analysis and dialectics within a system of differentiated terms.
A historical example for the connection between philosophy and religion is Baruch Spinoza’s Ethica, which was published in the 17th century [Spinoza]. The Ethica stands in the tradition of stoicism and can be seen as a guidebook for philosophical self-therapy [Hampe 2006]. Samuel Alexander has rightly applied the term “natural piety” for one of the therapeutic goals of this philosophy: by understanding that there are universal laws of nature that govern everything and by accepting that the power of any individual existing is much less than the power of nature as a whole it is possible, according to Spinoza, to develop happiness [Alexander 1939]. Its root is love for the impersonal god or for natural necessity as the universal condition of all activity, including one’s own.
Similar to the Hellenistic therapies [Hadot 2004] the Ethica emerged from the conflict between a religious and a critical-rational worldview. And similarly a contemporary philosophical therapy has to deal with the loss of orientation and sense that is created by the loss of religious dogmas [Van Hooft 2003, 22]. Complete physical and social well-being – as propagated by the World Health Organisation – is by all means no answer to the questions about aging and death. And in philosophy mental well-being cannot be “bought” by repressing transience [Wesche 2015, 12-24].
From a historical perspective the limits between philosophy, psychotherapy, science and religion are fluent and – except for the need to separate academic institutions and departments – there is no compelling reason why philosophical therapy could not remain an interdisciplinary project.
1. Achenbach Gerd (2010), Zur Einführung der Philosophischen Praxis, Dinter, Köln
2. Aizawa Kuniko, Atsushi Asai, Seiji Bito (2013), Defining futile life-prolonging treatments through Neo-Socratic Dialogue, BMC Medical Ethics 14:51, London
3. Alexander Samuel (1939), Natural Piety, in: Alexander Samuel, Philosophical and Literary Pieces, London & New York, 299-315
4. Banicki Konrad (2014), Philosophy as Therapy – Towards a Conceptual Model, Philosophical Papers, Vol.43, No.1, 7-31
5. Baus Lothar (2006), Die Philosophie des Buddha, in Buddhismus und Stoizismus: Zwei nahverwandte Philosophien und ihr gemeinsamer Ursprung in der Samkhya-Lehre, II. Auflage, Asclepios Edition, Homburg
6. Beckwith Christopher I. (2015), Greek Buddha: Pyrrho's Encounter with Early Buddhism in Central Asia. Princeton University Press, Princeton
7. Benatar David (2006), Better Never to Have Been: The Harm of Coming Into Existence, Oxford University Press
8. Bentley Jerry (1993), Old World Encounters: Cross-Cultural Contacts and Exchanges in Pre-Modern Times, Oxford University Press, New York
9. Bostrom, Nick (2005). A History of Transhumanist Thought, Journal of Evolution and Technology, 14 (1):1-25, Connectiut
10. Cavell Stanley (2004), Cities of Words, Harvard University Press
11. Contestabile Bruno (2014), Negative Utilitarianism and Buddhist Intuition, Contemporary Buddhism, Vol.15, Issue 2, 298-311, Routledge, London
12. Delmonte, M.M. (1984), Psychometric Sources and Meditation Practice: A Literature Review, Personality and Individual Differences, 5: 589-563
13. Devereux Georges (1974), Normal und Abnormal, Aufsätze zur allgemeinen Ethnopsychiatrie, Suhrkamp Verlag, Frankfurt
14. Epicurus, Letters to Meneoceus, ed. Withney Oates, New York, 1940
15. Freud Sigmund (1933), A Philosophy of Life, New Introductory Lectures on Psychoanalysis, Hogarth Press, London
16. Gethin Rupert (1998), Foundations of Buddhism, Oxford University Press
17. Goleman Daniel (1996), The Meditative Mind, Los Angeles Tarcher
18. Hadot Pierre (1995), Philosophy as a way of life, Blackwell, Oxford
19. Hadot Pierre (2004), What Is Ancient Philosophy?, Second Ed., Harvard
20. Hampe Michael (2006), Baruch de Spinoza: Ethik in geometrischer Ordnung dargestellt, Akademie Verlag, Berlin
21. Hampe Michael (2006), Psychoanalyse als antike Philosophy. Stanley Cavells Freud, in: Nach Feierabend 2, Zürich
22. Hampe Michael (2010), Rationality as Self-liberation in Spinoza´s Ethics, in: Journal of the Royal Institute of Philosophy 85. Supplement 66, 35-49
23. Harbsmeier Martin & Möckel Sebastian (2009), “Antike Gefühle im Wandel”, in: Pathos, Affekt, Emotion, Berlin Suhrkamp,
24. Harper Douglas (2015), Online Etymology Dictionary, available from http://www.etymonline.com
25. Höffe Otfried, Hrsg.(2006), Nikomachische Ethik, Akademie Verlag, Berlin
26. Hettlage Robert (2002), Generative Glückserfahrungen, in Glücksforschung - eine Bestandesaufnahme von Alfred Bellebaum (Ed.), UVK Verlag, Konstanz
27. Kahn Charles H. (1997), Plato and the Socratic Dialogue, Cambridge University Press
28. Kriz Jürgen (2000), Perspektiven zur ”Wissenschaftlichkeit” von Psychotherapie. Erschienen in: Hermer, Matthias (Hrsg): Psychotherapeutische Perspektiven am Beginn des 21 Jahrhunderts, 43-66, DGVT-Verlag, Tübingen
29. Kuzminski Adrian (2008), Pyrrhonism. How the Ancient Greeks reinvented Buddhism, Lanham
30. Laertius Diogenes (3rd century AD), Lives of Eminent Philosophers, William Heinemann, London, 1925
31. Lelkes Orsolya (2008), Happiness Across the Life Cycle: Exploring Age-Specific Preferences, European Centre for Social Welfare Policy and Research, Policy Brief, March (2), Wien
32. Lorenz Kuno (1998), Indische Denker, München.
33. Marinoff Lou (1999), Plato not Prozac! New York, Harper Collins, New York
34. McEvilley Thomas (2002), The Shape of Ancient Thought: Comparative Studies in Greek and Indian Philosophies, Allworth Press, New York
35. Nietzsche Friedrich (1885), Der Wille zur Macht, Albert Kröner Verlag, Stuttgart, 1964
36. Nussbaum Martha (1994), The Therapy of Desire, Princeton University Press, New Jersey
37. Overholser, James C. (1993). Elements of the Socratic method: Systematic Questioning, Psychotherapy, Vol.30, No.1, 67-74.
38. Raabe, Peter (2001), Philosophical Counseling, Praeger Publishers, Westport
39. Ritter Joachim & Gründer Karlfried (1998), Artikel “Therapie / Therapeutik” (by K. E. Rothschuh) in: Historisches Wörterbuch der Philosophie. Band 10, Darmstadt
40. Robertson Donald (2010), The Philosophy of Cognitive-Behavioral Therapy, Karnac, London
41. Robertson Donald (2013), Teach yourself Stoicism and the Art of Happiness, Hodder and Stoughton, London
42. Scheffler Samuel (2015), Der Tod und das Leben danach, Suhrkamp Verlag, Berlin
43. Smith, J.C. (1975), Meditation as Psychotherapy: A Review of the Literature. Psychological Bulletin 82: 558-64, University of Illinois
44. Spinoza Baruch (1677), Ethica ordine geometrico demonstrata. Hrsg. Wolfgang Bartuschat, Felix Meiner Verlag, Hamburg 1999
45. Spinoza Baruch (2002), Spinoza, Complete Works. Ed. By Michael L. Morgan, Indianapolis & Cambridge
46. Schuster Shlomit (1999), Philosophy Practice, Praeger Publishers, Westport
47. Segal Z., Williams M., Teasdale J. (2001), Mindfulness-Based Cognitive Therapy for Depression, The Guilford Press, New York
48. Taylor C.C.W.(1998), Socrates, Oxford University Press
49. Van Deurzen, E. (2002), Existential Counseling and Psychotherapy in Practice, Sage publications, London
50. Van Hooft Stan (2003), Philosophy as Therapy, Deakin University, Melbourne, available from www.existentialistmelbourne.org
51. Wesche Tilo (2015), Glück und Zeit, Eine formale Konzeption des guten Lebens,, in: Anghern Emil & Küchenhoff Bernd (eds.), Das unerledigte Vergangene. Macht und Grenzen der Erinnerung, Frankfurt a. M.: Velbrück
52. Zimmer Heinrich (1973), Philosophie und Religion Indiens, Suhrkamp Taschenbuch Wissenschaft, 7.Auflage 1992, Suhrkamp Verlag, Berlin
1. Philosophy as Therapy – Conceptual Models
2. Indian Sources of Hellenistic Ethics
3. Moral Perfectionism and Justice [German]
4. The Good Life in Philosophical Films